In this interview, our partner radiation oncologist Dr. David Kuczer speaks with Maja Zakarija—a Certified Medical Travel Professional and Austria-accredited Pharmaceutical Representative—about the biggest challenges international patients face when seeking cancer treatment abroad, and how Amethyst Radiotherapy Austria provides individualised, timely care tailored to each individual patient.
Dr. Kuczer also explains how modern radiotherapy is advancing cancer treatment: for selected indications, outcomes comparable to surgery can be achieved in 3–8 short sessions (~10 minutes each) over the course of approximately 1.5 weeks, without a scalpel or anaesthesia. Suitability is always assessed by our multidisciplinary team.
▶ Watch the full interview
https://amethyst-radiotherapy.at/wp-content/uploads/2025/10/Kuzcer-Interview-Austria.jpg720719webinar-adminhttps://amethyst-radiotherapy.at/wp-content/uploads/2023/09/AmethystWhiteLogo.pngwebinar-admin2025-10-08 09:00:122025-12-03 19:15:32Interview with Dr. David Kuczer — Fast Access to Advanced, Personalised Treatment
Transforming Cancer Treatment in Austria—With Precision and Compassion
At Amethyst Radiotherapy Austria, we understand that a cancer diagnosis can be life-changing—for both patients and their families. That’s why we are committed to delivering fast, accurate, and non-invasive treatment using state-of-the-art radiosurgery technologies, supported by a compassionate, patient-first approach. As part of the 30th anniversary celebrations at Wiener Privatklinik (WPK), Dr David was invited to speak about our pivotal role in shaping the future of tumour care in Austria.
▶ Watch the full interview to hear Dr David Kuczer share how we integrate innovation, medical expertise, and patient care to improve lives.
Why Patients Choose Amethyst Radiotherapy Austria
Our centre specialises in stereotactic radiosurgery (SRS)—a technique that delivers precisely focused radiation to tumours while minimising exposure to surrounding healthy tissue. This advanced, non-invasive alternative to traditional surgery avoids the need for incisions, hospitalisation, or prolonged recovery.
As Dr David outlines, our approach to care is built on four key pillars:
Pinpoint Tumour Location
We use advanced diagnostic imaging systems—including MRI, CT, and PET scans—to map tumours with millimetre-level accuracy.
Non-Invasive Treatment Delivery
Our Elekta Versa HD linear accelerator delivers highly targeted radiation without any surgical intervention.
Rapid Access to Treatment
With no long waiting lists, we offer same-day consultation and treatment planning, ensuring timely care.
Tailored Treatment Pathways
Each patient benefits from a personalised care plan, based on their specific diagnosis and medical needs.
Our Centre Within WPK, Powered by Amethyst
Situated within Wiener Privatklinik (WPK)—Austria’s only private hospital—Amethyst Radiotherapy Austria merges WPK’s exceptional clinical environment with Amethyst’s expertise in advanced, non-invasive tumour care. As part of the Amethyst Healthcare Group—one of Europe’s largest and most experienced radiotherapy providers—we deliver internationally recognised cancer care standards with the personalised attention of a local specialist team.
Take the Next Step Towards Personalised Cancer Care
We are committed to offering bespoke cancer treatment tailored to each individual’s needs. From initial consultation to treatment and follow-up, every stage is guided by precision, compassion, and efficiency. Combining medical innovation with human understanding, our expert team provides rapid access to trusted, non-invasive tumour care in a calm, professional, and supportive environment you can rely on.
https://amethyst-radiotherapy.at/wp-content/uploads/2025/06/Screenshot-2025-06-12-114312.png10781918Jenny Leehttps://amethyst-radiotherapy.at/wp-content/uploads/2023/09/AmethystWhiteLogo.pngJenny Lee2025-06-12 10:49:242026-03-21 17:56:47Dr. David Kuczer Discusses Advanced Tumour Care at Amethyst Austria
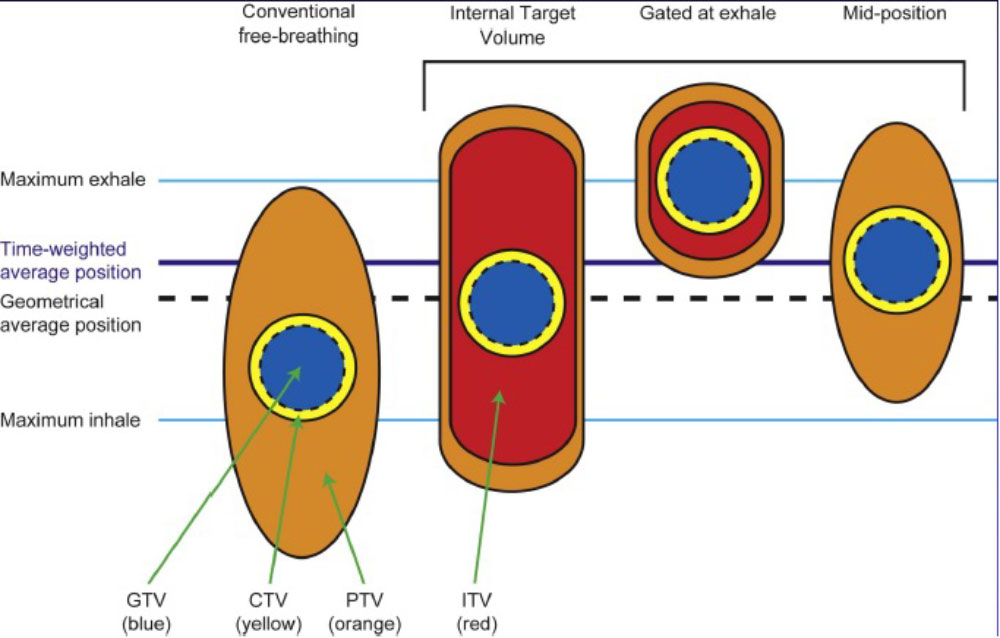
Conventional (ITV-based) – Contour and treat full tumor ROM
Accelerator beam gating – Patient breathes normally; beam only on while patient is in a certain phase of the respiratory cycle
Active breathing control – Patient holds breath in a certain position; beam only on in that phase of the respiratory cycle
Dynamic tumor tracking – Patient breathes normally; tumor is tracked; beam always on and moves with tumor
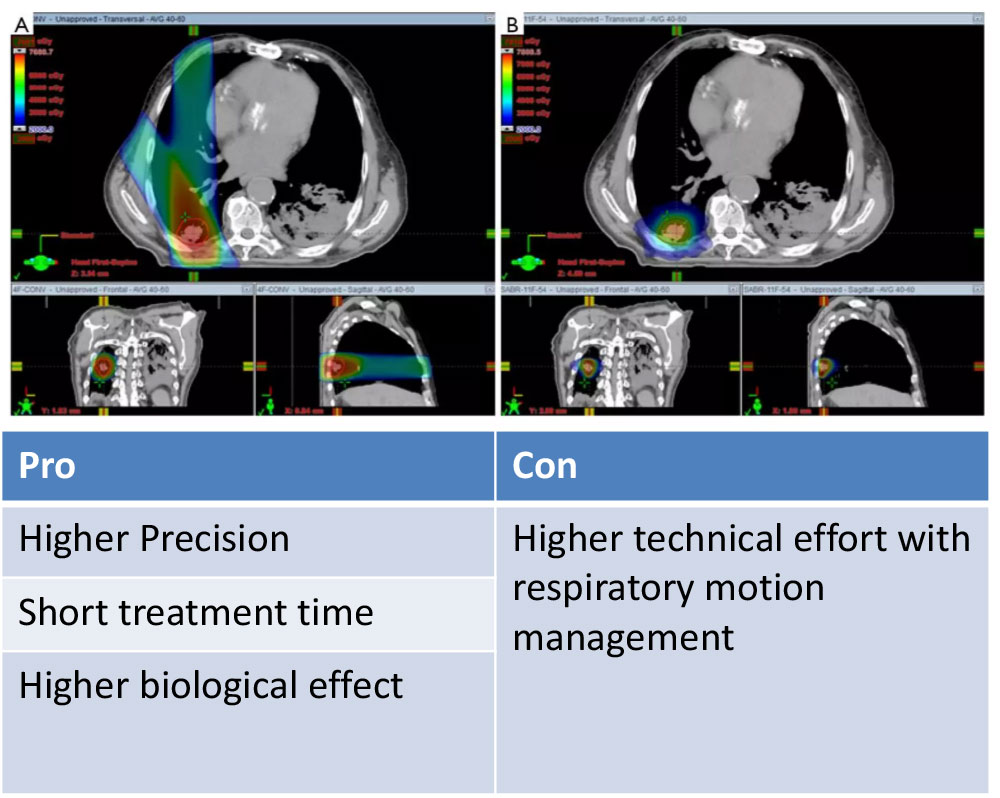
Regardless of the motion management used, an additional “CTV/PTV” margin around our target is needed to ensure that we hit it.
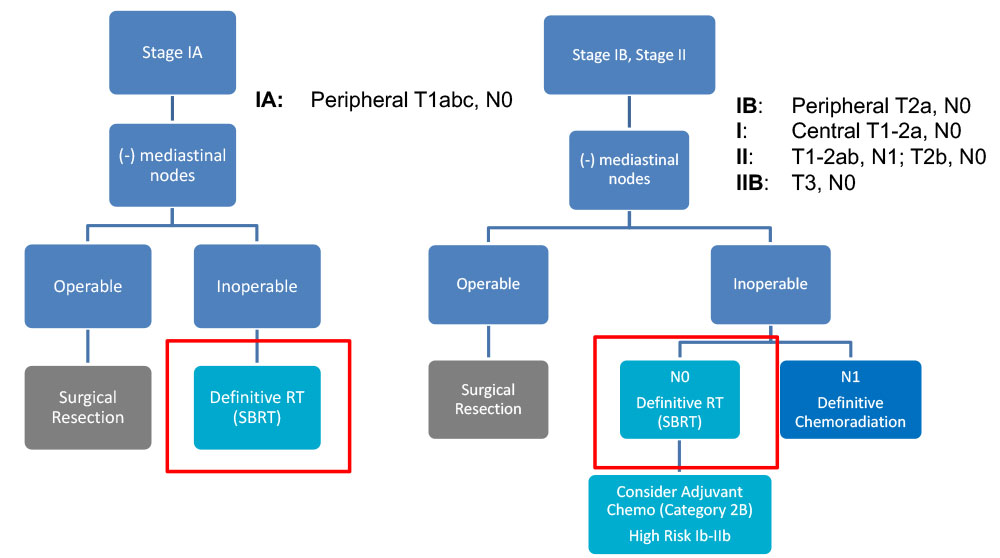
Curative Indication - NCCN Guidelines – NSCLC
Curative Indication - NCCN Guidelines – NSCLC
Surgical resection is the preferred local treatment
– An anatomical resection with lobectomy or segmentectomy is preferred to wedge resection
– Includes sampling of at-risk ipsilateral hilar and mediastinal LN
SBRT for patients who are medically inoperable orrefuse surgery –Limitations: High volume (DM > 5cm) and “ultra-central” tumors should be treated more cautiously (e.g. 10 instead of 3 fractions)
–Limited data yet supporting the addition of systemic therapy to SBRT
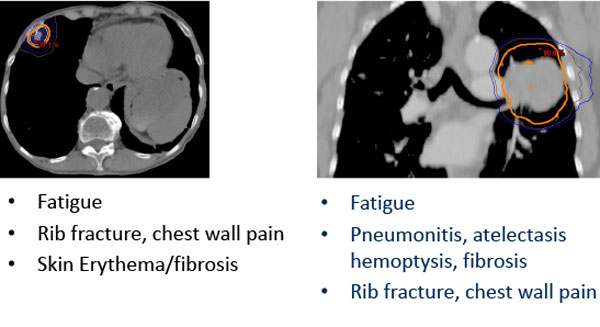
Potential SBRT Toxicity Depends on Tumor Site
Risk of toxicity can be reduced through risk-adapted dose-fractionation
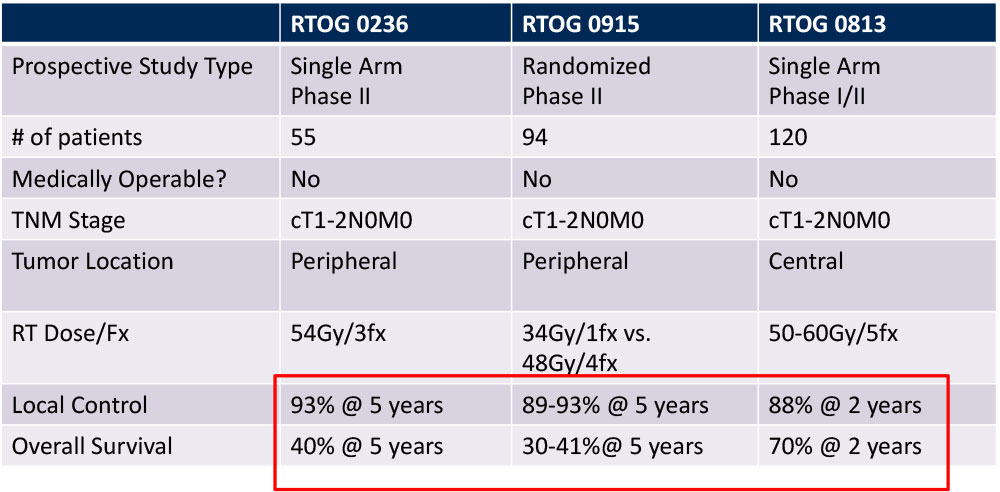
Outcomes of SBRT for Early Stage NSCLC
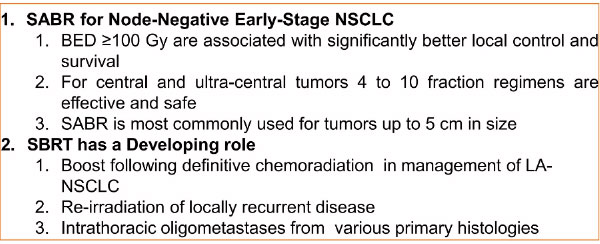
Take Home Pearl and Further Indications of SBRT for NSCLC
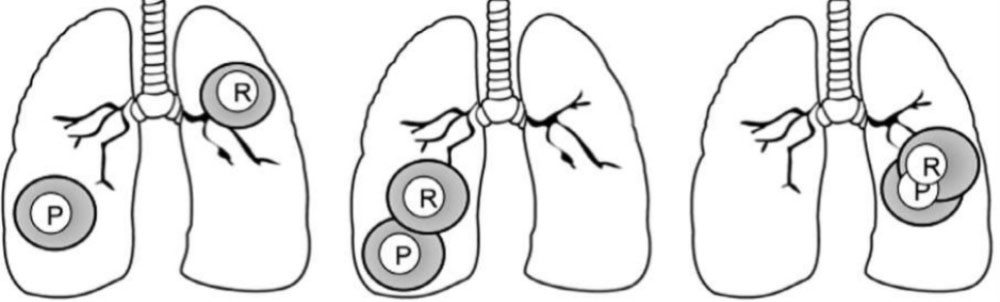
Reirradiation of Recurrent disease
Feasibility of treating with curative intent depends on site of primary (P) and recurrent (R) tumors
Advanced treatment techniques are particularly useful for sparing normal tissue (e.g., IMRT, SBRT, protons)
– Reirradiating central structures (e.g., esophagus, airway) most challenging
– Long-term toxicity is the major concern – impacted by dose/fraction
Dyspnea/Dysphagia
–Tumor obstruction causing SVC, respiratory distress or esophageal narrowing
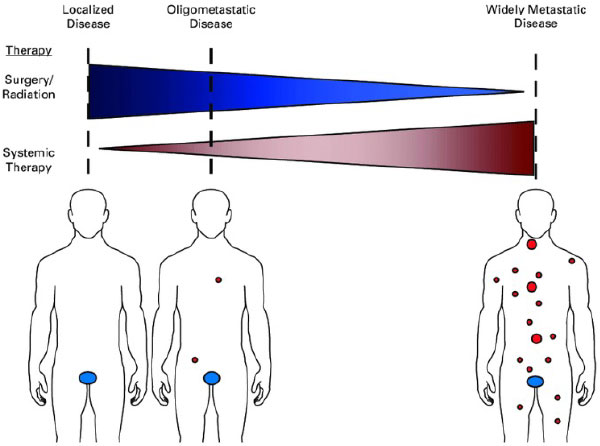
Is all metastatic disease the same?
No! Lung cancer has M1a, M1b and M1c designations because the metastatic state at diagnosis impacts prognosis; a small subset of patients may be cured
“Oligometastatic” refers to a situation where distant metastases may be limited in number (typically defined as < 5 mets in < 3 organs), and potentially curative treatment can be delivered prior to the development of widespread disease
UT Southwestern Randomized Phase II Trial
Iyengar et al, JAMA Oncol, 2018
29 patients, oligometastatic NSCLC with < 5 sites of disease (EGFR/ALK negative), PR or SD after induction chemo, randomized to +/- SAbR
SAbR à ↑ M-PFS (3.5à9.7mo)
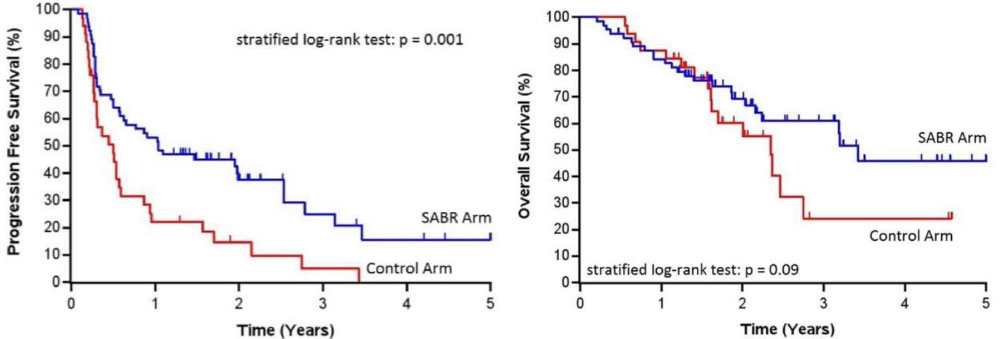
SABR-COMET Randomized Phase II Trial
Palma et al, Lancet, 2019
99 patients, variety of oligometastatic cancers with < 5 sites of disease, PR/SD on systemic therapy, randomized 1:2 to +/- SAbR (at ablative doses)
– Most common histologies: breast, lung, colorectal, prostate
SAbR à ↑ M-PFS (6à12mo, p<0.001) & M-OS (28à41mo, p=0.09)
– Also ↑ G2 or higher toxicity, but no difference in QOL
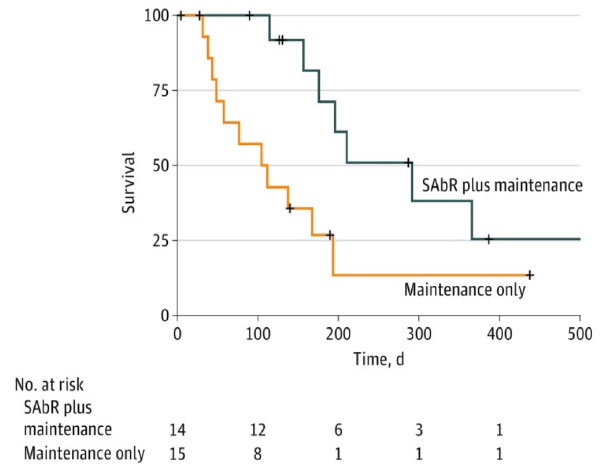
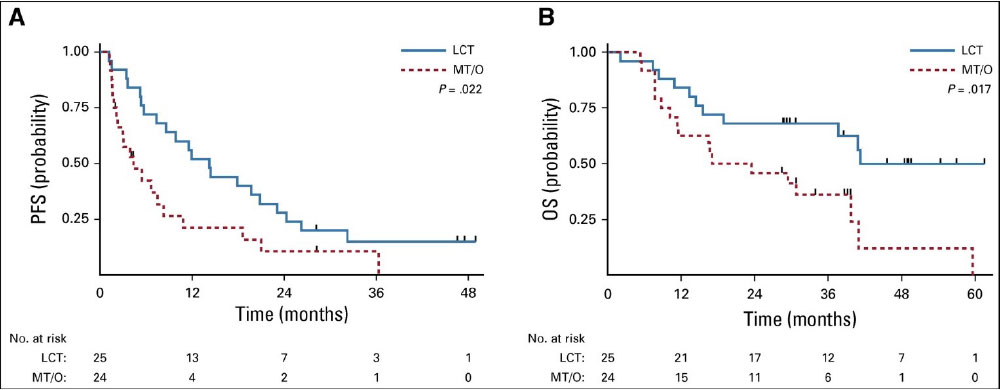
Multi-Institutional Randomized Phase II Trial
Gomez et al, J Clin Oncol, 2019
49 patients with oligometastatic NSCLC with < 3 sites of disease, SD/PR after Pt-based doublet or EGFR/ALK inhibitor, randomized to maintenance systemic therapy +/- local consolidative surgery/RT
RT à ↑ M-PFS (4.4à14.2mo) and M-OS (17à41mo, p=0.02)
The Future…
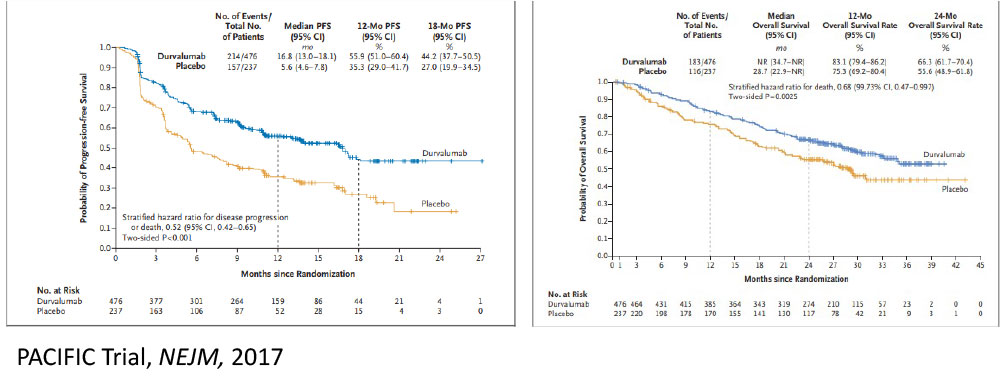
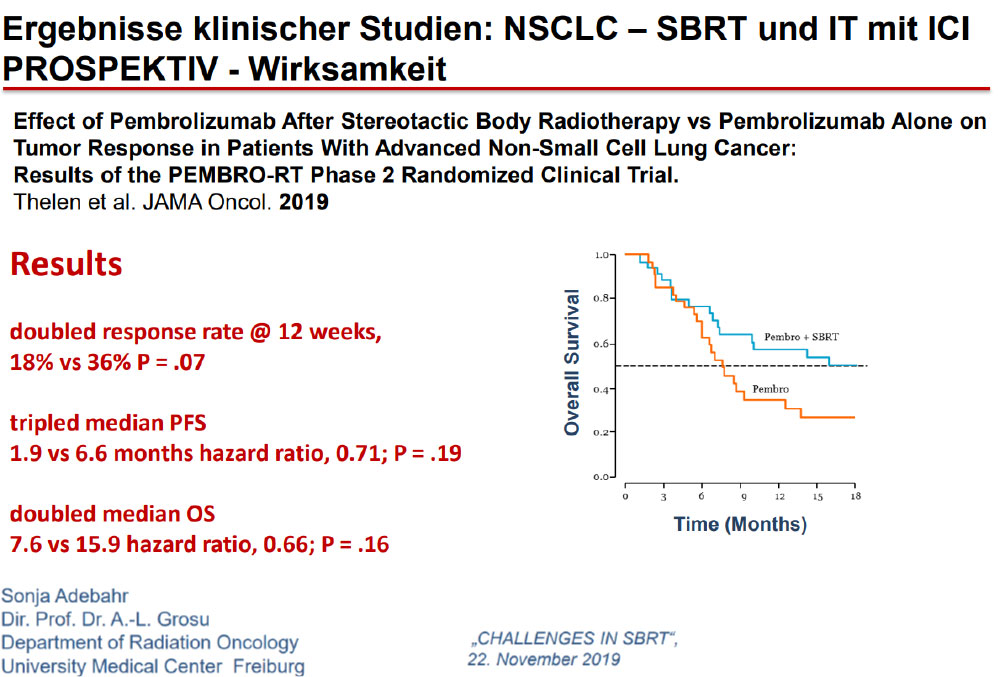
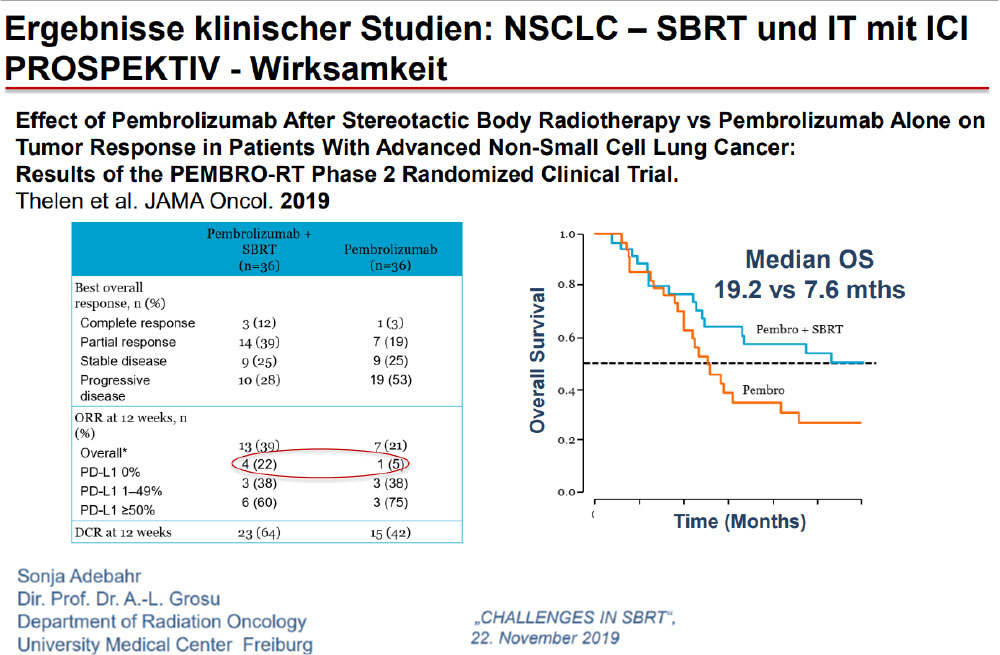
Immunotherapy May Change Our Approach to Locoregional Management Too
A stronger immune response may be elicited by leaving a tumor in and irradiating it, rather than removing the largest source of antigenic stimulation.
The Future……Aktive Protokolle
PACIFIC-4 / RTOG 3515
Inclusion Criteria
Clinical Stage I/II node negative (T1 – T3 N0)
Medically inoperable or refuse surgery
ECOG PS 0-2
All comers for histology and PDL-1 status
Sync/Metach allowed
The Future…A Few Examples of Active Clinical Trials in Lung Cancer
CAVE: Not all new substances proofed to be safe with SBRT. Additional surveys needed!
NRG LU002: Adds RT (to all sites of disease) to systemic therapy for oligometastatic NSCLC
NRG LU004: Adds immunotherapy to IMRT or 3-D CRT for stage II-III NSCLC with high PD-L1 expression (instead of chemotherapy)
PACIFIC 4 and NRG/S1914: Adds consolidative immunotherapy to SBRT for stage I NSCLC
AEGEAN: Adds neoadjuvant immunotherapy to surgery for resectable stage II-III NSCLC
ALCHEMIST: Evaluating adjuvant use of targeted agents for resected NSCLC
RTOG 1308: Compares proton therapy to photon therapy for LA-NSCLC
NRG LU005: Adds immunotherapy to chemoradiation for limited-stage SCLC
NRG CC003: Hippocampal avoidance PCI for SCLC
Quellen
David S. Buchberger et al. Stereotactic Body Radiotherapy for the Management of Early-Stage Non–Small-Cell Lung Cancer: A Clinical Overview. JCO Oncol Pract 19, 239-249(2023).DOI:10.1200/OP.22.00475
https://amethyst-radiotherapy.at/wp-content/uploads/2022/04/CancerTypes.jpg533800webinar-adminhttps://amethyst-radiotherapy.at/wp-content/uploads/2023/09/AmethystWhiteLogo.pngwebinar-admin2024-04-26 00:12:592026-03-21 17:57:25SBRT bei NSCLC (Dr David Kuczer – 2024)
Radiotherapy uses high-energy beams to kill prostate cancer cells. It is a treatment option for nearly all cancer stages, from early-stage tumours to more advanced and metastatic prostate cancer.
Our radiation oncology team at Amethyst Radiotherapy, represents the largest pan-European network of high-tech radiotherapy centres. Our doctors are committed to providing cutting-edge radiation therapy treatments that effectively target cancer while minimising the risk of side effects. One of these innovative methods is hydrogel spacers.
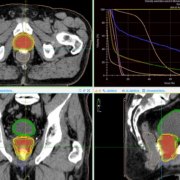
This technique involves the use of an absorbable gel that temporarily creates a gap between the prostate and rectum, significantly reducing the risk of bowel radiation during treatment. Hydrogel spacers also improve tumor targeting, reducing the total number of treatment sessions from 39 to 7.
This means that you can complete your treatment in 2.5 weeks instead of 8 weeks. The method is used for localised prostate cancer and is performed on an outpatient basis every 2nd working day. A treatment takes about 10 minutes and is painless.
Attached is the example of the first patient we treat using this method. You can see the dose by the very precise color that surrounds the prostate, as well as the white color of the spacer gel that pushes the rectum away from the prostate.
Radiation techniques available at Amethyst Radiotherapy include:
Image guided VMAT radiation therapy
Volumetric modulated arc therapy (VMAT) is one of the most advanced techniques of external radiotherapy. It involves the use of a linear accelerator machine that rotates around the patient while he lies down. The machine precisely delivers radiation doses to the tumor site while limiting the amount of radiation received by the healthy tissues surrounding it.
Stereotactic Body Radiotherapy (SBRT)
Amethyst Radiotherapy is among the few private centres in Europe offering SBRT radiotherapy, and the only one in Austria. SBRT is a cutting-edge radiotherapy technique that can comprise the radiotherapy treatment into a few sessions, by delivering higher radiation doses safely and efficiently. SBRT is an efficient treatment option both for metastasis/lymph nodes as well as for small PET positive relapses for patients that had radiotherapy previously.
https://amethyst-radiotherapy.at/wp-content/uploads/2023/05/ProstateRadiation.jpg9181509webinar-adminhttps://amethyst-radiotherapy.at/wp-content/uploads/2023/09/AmethystWhiteLogo.pngwebinar-admin2023-05-28 14:07:112025-07-15 11:50:58Stereotactic radiation of prostate cancer in 7 instead of 39 sessions